Originally published as:
Expanded Stem Cell Therapy as a Possible Alternative to Shoulder Surgery: MRI-Confirmed Healing of Rotator Cuff Tear – A Case Report
Kosmos Publishers, 2026
Author: Dr. Hassan Mubark
Original publication: Kosmos Publishers
Original URL: https://kosmospublishers.org/expanded-stem-cell-therapy-as-a-possible-alternative-to-shoulder-surgery-mri-confirmed-healing-of-rotator-cuff-tear-a-case-report-2/
Hassan Mubark*
Rheumatologist, Institution: Auckland Regenerative Clinic, Ormiston Specialist Centre, 125 Ormiston Road, Flat Bush, Auckland 2019, New Zealand
Received Date: December 12, 2025; Accepted Date: January 10, 2026; Published Date: January 22, 2026;
*Corresponding author: Hassan Mubark, Rheumatologist, Institution: Auckland Regenerative Clinic, Ormiston Specialist Centre, 125 Ormiston Road, Flat Bush, Auckland 2019, New Zealand. Phone: +64 9 2713305; Mobile: +64 21843513; Fax: +64 9 2770769; Email: drhassanmubark@gmail.com
DOI: 10.37722/AOASM.2026102
Watch the Article in Motion

Information Board
ISSN: 2641-6859
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Language:English
Impact Factor: 4.9
Abstract
Background: Partial-thickness supraspinatus tears and long-head biceps tendon pathology, including tenosynovitis, are common causes of shoulder pain and functional impairment. When conservative management fails, arthroscopic surgery is frequently recommended. Biologic therapies—particularly adipose-derived mesenchymal stem cells (AD-MSCs)—are emerging as minimally invasive regenerative alternatives.
Case: A 50-year-old male business development manager sustained an acute left-shoulder injury while twisting with a 10-kg lawn-mower catcher. He developed significant functional limitations, including restricted shoulder elevation, inability to reach behind his back, nocturnal pain, and reduced work capacity. Conservative treatments—including osteopathy, acupuncture, and corticosteroid injection—provided only transient relief. Baseline MRI demonstrated a 10-mm articular-surface partial-thickness supraspinatus tear, long-head biceps tenosynovitis, and subacromial bursitis. Surgical repair was scheduled.
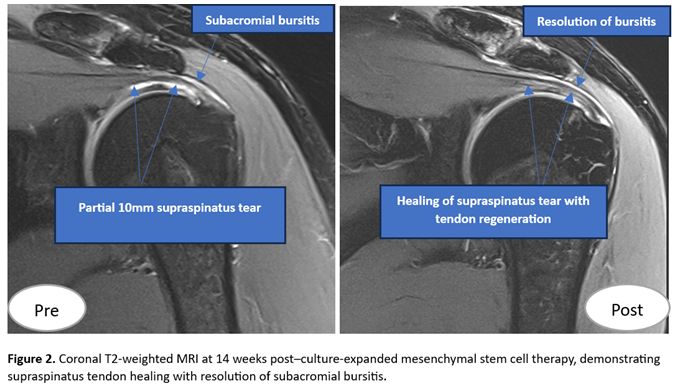
The patient underwent culture-expanded autologous adipose-derived MSC therapy. A structured rehabilitation program was implemented, consisting of light exercises during the first two weeks followed by progressive strengthening. At 14-week follow-up, the patient reported approximately 80% clinical improvement, returned to full work duties after only six days off, and cancelled the planned surgery. Follow-up MRI demonstrated healing of the supraspinatus tear with resolution of biceps tenosynovitis and subacromial bursitis.
Conclusion: This case demonstrates clinically meaningful improvement with MRI-documented healing of a partial-thickness supraspinatus tear, long-head biceps tendinitis, and subacromial bursitis following culture-expanded AD-MSC therapy, effectively avoiding shoulder surgery. Controlled studies are warranted to further evaluate efficacy and reproducibility.
Keywords: Adipose-derived mesenchymal stem cells; culture-expanded MSCs; partial-thickness rotator cuff tear; supraspinatus tendon; long-head biceps tenosynovitis; subacromial bursitis; orthobiologics; magnetic resonance imaging; regenerative medicine; shoulder surgery avoidance.
Introduction
Rotator cuff tears (RCTs) are common musculoskeletal conditions whose prevalence increases with advancing age, often reflecting progressive tendon degeneration rather than acute injury alone [1]. Many RCTs remain asymptomatic; however, when symptoms develop, patients may experience significant shoulder pain, weakness, and functional limitation affecting daily activities and quality of life [2]. Conventional non-operative treatments, including physiotherapy and subacromial corticosteroid injections, can provide symptomatic relief but do not address the underlying tendon pathology and often yield only short-term benefits [3].
Importantly, current non-surgical strategies are largely palliative, targeting pain modulation and functional compensation rather than restoring tendon structure or reversing degenerative changes. As a result, symptom recurrence and progressive tendon deterioration are common, particularly in chronic and biologically compromised tears.
Chronic rotator cuff tears demonstrate limited intrinsic healing capacity, making spontaneous structural repair unlikely and frequently leading to recommendations for surgical intervention in symptomatic cases [4]. Despite advances in surgical techniques, re-tear rates and incomplete tendon–bone healing remain substantial challenges, particularly in degenerative and chronic tears, and surgical outcomes may be suboptimal in older patients or those with poor tendon quality [5].
These limitations have driven increasing interest in regenerative medicine strategies, including platelet-rich plasma (PRP) and mesenchymal stem cell (MSC)–based therapies, aimed at enhancing biological tendon repair rather than relying solely on mechanical fixation or symptom control [6]. Preclinical studies have demonstrated that MSCs can promote tendon regeneration through paracrine signaling, modulation of inflammation, and improved tendon–bone interface healing [7]. Emerging clinical evidence suggests that stem cell–based therapies may improve pain, function, and structural healing in selected patients with rotator cuff tears, offering a promising biologic alternative or adjunct to surgical repair [8].
Rotator cuff tears are associated with a biologically compromised tendon–bone interface and reduced local regenerative capacity. Reduced concentrations of mesenchymal stem cells at the greater tuberosity have been demonstrated in symptomatic rotator cuff tears, suggesting an intrinsic impairment in tendon healing [9]. This has led to increasing interest in biologic augmentation, with clinical studies showing improved pain and functional outcomes following autologous bone marrow–derived cell therapies [10]. Randomized controlled trial data further support the potential benefit of bone marrow concentrate, alone or combined with platelet products, as a non-surgical regenerative treatment for rotator cuff tears [11].
Case Report
Patient and Injury
A 50-year-old right-handed business development manager injured his left shoulder when twisting with a 10-kg lawn-mower catcher, hearing an audible snap and fearing dislocation.
Symptoms
• Inability to lift arm above 90°
• Difficulty reaching behind his back
• Severe nocturnal pain
• Pain with lifting and reduced work capacity
Baseline MRI Findings
• 10-mm supraspinatus articular-surface partial-thickness tear
• Long-head biceps tenosynovitis
• Subacromial bursitis
• Mild glenohumeral joint (GHJ) and acromioclavicular (ACJ) osteoarthritis, labral fraying, loose body
Intervention: Culture-Expanded AD-MSC Therapy
Adipose tissue was harvested, and mesenchymal stem cells (MSCs) were culture-expanded using the following protocol. After obtaining informed consent, abdominal subcutaneous adipose tissue was collected by a qualified plastic surgeon under sterile conditions. The harvested lipoaspirate was washed and enzymatically digested using collagenase (0.2 U/mL). The resulting stromal vascular fraction (SVF) was isolated by density-gradient centrifugation and subsequently plated for culture expansion. Cells were cultured in Dulbecco’s Modified Eagle Medium (DMEM) supplemented with 10% human platelet lysate (HPL) to promote MSC proliferation. The cells were expanded to approximately 90% confluency over a period of just under six weeks, after which they were cryopreserved until the scheduled treatment date.
On the day of administration, the cryopreserved cells were thawed, washed, and filtered under sterile conditions, then resuspended in Hartmann’s solution supplemented with 10% HPL and prepared in syringes for injection. Cell counts were determined manually using a haemocytometer, and cell viability was assessed by trypan blue exclusion dye assay.
Ultrasound-guided injections performed:
1. Intra-articular GHJ: 50 million MSCs + platelet-rich plasma (PRP) + soluble hyaluronic acid (HA) to protect the joint and slow the progression of mild osteoarthritis
2. Supraspinatus tendon substance directly into the tear: 25 million MSCs + PRP (fig1) and vid 1
3. Subacromial bursa: 25 million MSCs + PRP
4. Biceps tendon sheath: 25 million MSCs + PRP
5. Subscapularis tendon: 25 million MSCs + PRP

Video 1 demonstrating stem cells into the supraspinatus tendon tear under ultrasound guidance. (click here to watch)
Outcomes
Clinical Outcomes at 14 Weeks
A structured rehabilitation program was implemented, consisting of light exercises during the first two weeks followed by progressive strengthening
• ~80% pain and function improvement
• Returned to full work duties
• Surgery was cancelled
MRI Findings at 14 weeks (Fig.2)
• No visible supraspinatus defect
• Minimal residual insertional interstitial signal
• Resolution of subacromial bursitis
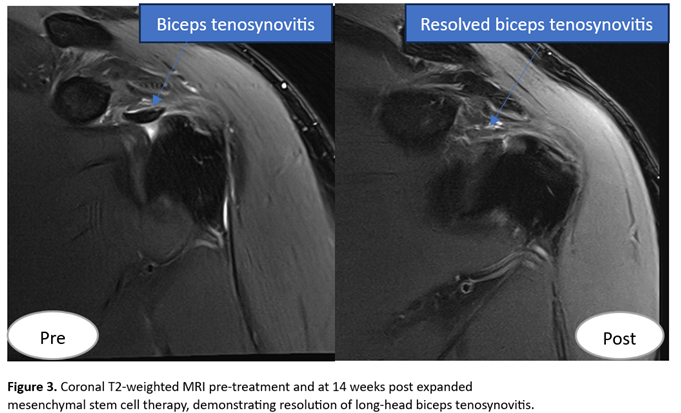
• Resolution of long-head biceps tenosynovitis with normal tendon continuity and groove position (Fig.3)
Discussion
Rotator cuff tendons are prone to degeneration due to limited vascularity and a reduced intrinsic regenerative capacity, resulting in poor healing responses following injury and a tendency toward fibro-scar formation rather than true tendon regeneration [12]. This biological limitation underpins the high failure and re-tear rates observed with both conservative care and surgical repair, particularly in degenerative supraspinatus pathology [13].
Regenerative medicine strategies aim to biologically augment tendon repair by providing cellular and molecular signals that promote neotendon formation rather than mechanically inferior scar tissue [14]. Mesenchymal stem cells (MSCs) have emerged as a promising modality due to their paracrine activity, immunomodulatory effects, and ability to influence tenocyte differentiation and extracellular matrix remodeling [15].
In parallel, platelet-rich plasma (PRP) delivers a concentrated milieu of growth factors that support angiogenesis, cellular recruitment, and matrix synthesis, making it a logical biological adjunct for tendon healing [16]. The combined use of MSCs and PRP is hypothesised to exert synergistic effects, whereby PRP enhances stem cell viability and signaling while MSCs provide sustained regenerative cues within the damaged tendon environment [17].
In the present case, a partial-thickness supraspinatus tendon tear demonstrated both clinical improvement and radiological evidence of tendon healing following a single, ultrasound-guided, non-surgical injection of combined autologous stem cells and PRP [18]. Importantly, this regenerative response was accompanied by complete resolution of associated subacromial bursitis, suggesting that the biologic intervention addressed not only the tendon defect but also the inflammatory peritendinous milieu [19].
The resolution of subacromial bursitis is clinically relevant, as bursitis is a major contributor to pain, impingement symptoms, and functional limitation in rotator cuff disease, and its persistence often predicts poor outcomes with standard conservative therapies [20]. The ability of biologic therapy to simultaneously modulate inflammation and promote structural repair highlights a potential advantage over isolated physical therapy, corticosteroid injection, or analgesic-based approaches.
This case builds upon our previously published world-first report of complete MRI-confirmed healing of a full-thickness, retracted supraspinatus tendon tear treated non-surgically using expanded autologous adipose-derived stem cells, achieving an outcome comparable to surgical repair [21]. While the current case involves a partial-thickness tear, it reinforces the concept that biologic tendon regeneration is achievable across the rotator cuff disease spectrum, from early-stage partial tears to advanced full-thickness retracted pathology. Together, these cases support the evolving paradigm that selected rotator cuff tears can be biologically healed rather than mechanically repaired.
Despite the encouraging outcomes, limitations include the single-case design and the absence of histological confirmation of neotendon formation, which restricts generalisability and mechanistic certainty [12]. Nevertheless, adherence to established regulatory frameworks and biologics reporting standards strengthens the clinical relevance of these findings [20].
Conclusion
Culture-expanded AD-MSC therapy resulted in marked clinical improvement and MRI-confirmed healing of the supraspinatus tear and long-head biceps pathology, thereby avoiding the need for surgery. Larger, controlled clinical studies are required to validate and extend these promising findings.
Patient Consent: Written informed consent was obtained for publication.
Acknowledgement: The authors thank the patient for consenting to share his case in support of advancing regenerative science and acknowledge the radiologist for providing detailed reports and high-quality pre- and post-treatment MRI images.
References
- Minagawa H, Yamamoto N, Abe H, Fukuda M, Seki N, Kikuchi K, et al. Prevalence of symptomatic and asymptomatic rotator cuff tears in the general population: a cross-sectional study. J Orthop Sci. 2013;18(5):741–746.
- 2.Sambandam SN, Khanna V, Gul A, Mounasamy V. Rotator cuff tears: an evidence-based approach. World J Orthop. 2015 Dec 18;6(11):902–918.
- 3.Blair B, Rokito AS, Cuomo F, Jarolem K, Zuckerman JD. Efficacy of injections of corticosteroids for subacromial impingement syndrome. J Bone Joint Surg Am. 1996;78(11):1685–1689.
- Safran O, Schroeder J, Bloom R, Weil Y, Milgrom C. Natural history of nonoperatively treated symptomatic rotator cuff tears in patients 60 years old or younger. Am J Sports Med. 2011 Apr;39(4):710–4.
- 5.Han L, Fang WL, Jin B, et al. Enhancement of tendon–bone healing after rotator cuff injuries using combined therapy with mesenchymal stem cells and platelet-rich plasma. Eur Rev Med Pharmacol Sci. 2019;23(20):9075–9084.
- 6.Kim SJ, Song DH, Park JW, et al. Effect of bone marrow aspirate concentrate–platelet-rich plasma on tendon-derived stem cells and rotator cuff tendon tear. Cell Transplant. 2017;26(5):867–878.
- Ding DC, Shyu WC, Lin SZ. Mesenchymal stem cells. Cell Transplant. 2011;20(1):5–14.
- 8.Charles MD, Christian DR, Cole BJ. The role of biologic therapy in rotator cuff tears and repairs. Curr Rev Musculoskelet Med. 2018;11(1):150–161.
- Hernigou P, Merouse G, Duffiet P, Chevallier N, Rouard H. Reduced levels of mesenchymal stem cells at the tendon–bone interface tuberosity in patients with symptomatic rotator cuff tear. Int Orthop. 2015 Mar;39(6):1219–1225.
- Centeno CJ, Al-Sayegh H, Bashir J, Goodyear S, Freeman MD. A prospective multi-site registry study of a specific protocol of autologous bone marrow concentrate for the treatment of shoulder rotator cuff tears and osteoarthritis. Pain Res Manag. 2015;8:269–276.
- Centeno CJ, Fausel Z, Stemper I, et al. A randomized controlled trial of the treatment of rotator cuff tears with bone marrow concentrate and platelet products compared to exercise therapy: a midterm analysis. Stem Cells Int. 2020;2020:5962354.
- Harrison-Brown M, Scholes C, Hafsi K, et al. Efficacy and safety of culture-expanded mesenchymal stem/stromal cells for the treatment of knee osteoarthritis: a systematic review protocol. J Orthop Surg Res. 2019;14:34.
- Centeno CJ, Al-Sayegh H, Freeman MD, et al. A multi-center analysis of adverse events among two thousand three hundred seventy-two adult patients undergoing autologous stem cell therapy for orthopaedic conditions. Int Orthop. 2016;40(8):1755–1765.
- Andia I, Maffulli N. Biological therapies in regenerative sports medicine. Sports Med. 2017;47(5):807–828.
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11–15.
- Foster TE, Puskas BL, Mandelbaum BR, Gerhardt MB, Rodeo SA. Platelet-rich plasma: from basic science to clinical applications. Am J Sports Med. 2009;37(11):2259–2272.
- Tatsis D, Vasalou V, etal. The combined use of platelet-rich plasma and adipose-derived mesenchymal stem cells promotes healing: a review of experimental models and future perspectives. Biomolecules. 2021;11(10):1403.
- Kim YS, Sung CH, Chung SH, Kwak SJ, Koh YG. Does an injection of mesenchymal stem cells loaded in fibrin glue influence rotator cuff repair outcomes? Am J Sports Med. 2017;45(9):2010–2018.
- Jo CH, Lee SY, Yoon KS, et al. Intratendinous injection of autologous adipose tissue-derived mesenchymal stem cells for the treatment of rotator cuff disease: a first-in-human trial. Stem Cells. 2018;36(9):1441–1450.
- Murray IR, Geeslin AG, Goudie EB, Petrigliano FA, LaPrade RF. Minimum Information for Studies Evaluating Biologics in Orthopaedics (MIBO): reporting guidelines for clinical studies. J Bone Joint Surg Am. 2017;99(10):809–819.
- Mubark H, et al. MRI-documented tendon healing following expanded autologous adipose-derived cell therapy for rotator cuff pathology: a clinical case report. Biologic Orthop J. 2023;1(1):7–10.
Author note: This article was authored by Dr. Hassan Mubark, who is also the clinical director of Regenerative Clinic NZ. Republishing is permitted by the author.
Medical Disclaimer: This article is a case report and is provided for educational purposes only. It does not constitute medical advice. Individual results may vary. Patients should consult a qualified medical professional before pursuing treatment.
Dr Hassan Mubark is an experienced joint disease specialist with more than 30 years in medical practice. Specializing in Rheumatology from 2007, he became particularly interested in musculoskeletal and sports medicine as well as regenerative medicine. For many years, he has worked in this field, starting with plasma (PRP) and then moving to autologous fat-derived expanded mesenchymal stem cell therapy with growing interest over the past few years.